
By Mirabel Pelton
My research asks why autistic people* [A] are more likely to engage in suicidal thoughts and behaviours than people who aren’t autistic. I want to produce evidence that will really reduce suicide rates. As I near the end of my second year as a PhD student, I’ve noticed that, when I introduce my research, people respond in one of two ways: they are either shocked and upset or not shocked at all. I’ll come back to this later but, for now, this blog outlines three current areas of concern: (i) rates of suicide amongst autistic people; (ii) how suicide models explain this; (iii) and how accurately we can assess risk. We need to focus on all three of these to reduce suicide rates.
1. Are autistic people at greater suicide risk than not autistic people?
Autism is a lifelong condition* [B] present from early childhood characterized by communication, social and sensory differences and a preference for sameness. Over the last decade research has consistently reported that autistic people are more likely to likely to think about, attempt and die by suicide. In the first study in my PhD, in a sample of 695 autistic and not autistic adults, 38% of autistic people reported at least one past suicide attempt versus 10% of not autistic people (submitted). There are now two large scale population studies, one of which reports a 9-fold increase in death by suicide amongst autistic adults without intellectual disability [1]. It is no longer in doubt that autistic people are at greater risk but these figures may still be an underestimation: Autism is typically diagnosed in childhood but women and girls, black and ethnic minority groups and older adults are much less likely to receive a diagnosis or the support they need. The true figures could be much higher as these people are ‘missed’.
2. Why are autistic people more likely to experience suicidal thoughts and behaviours?
Research has identified that, similar to the general population, autistic people who experience trauma or depression are more likely to engage in suicidal thought and behaviours. There’s also research describing how some risk factors may have a greater impact for autistic people, such as camouflaging autistic characteristics to appear less autistic and having unmet support needs [2]. However, we know such associations can be poor predictors of those most at risk; for example, most who experience depression won’t go on to die by suicide. My PhD explores how Joiner’s Interpersonal Theory of Suicide (ITS; 2005) might be useful to understand how suicidal thoughts and behaviours develop in autistic people [3]. I was struck by Joiner’s theory as it argues that interpersonal difficulties – a core characteristic of autism – appear to relate to suicidal behaviour in any population group. Autistic people regularly report that they lack independence and control over their own lives (indicating ‘burdensomeness’ within the model) or feel isolated (indicating ‘thwarted belonging’) and this impacts their mental health and quality of life. Autistic people more frequently report lifetime trauma (e.g., abuse as a child or adult, being homeless or evicted from home) [4] than not autistic people and, according to the ITS, this would make them much more vulnerable to a suicide attempt.
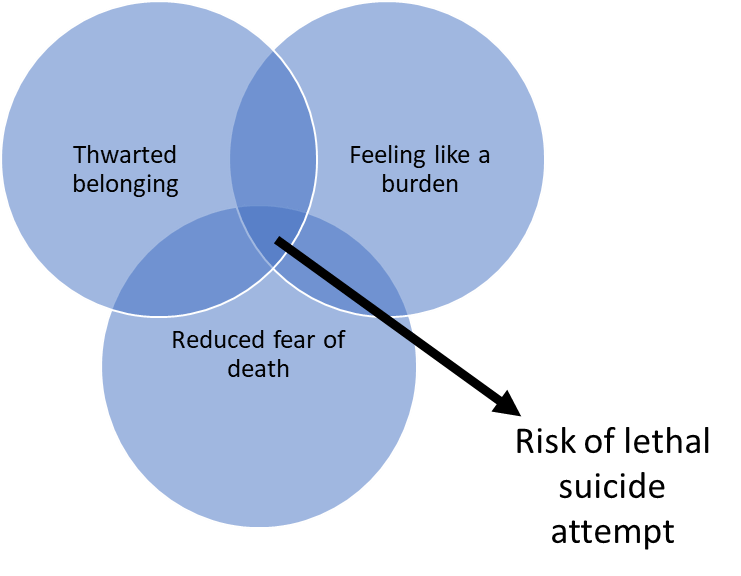
I’ve compared the ITS in autistic and not autistic people and the findings are surprising: as expected, autistic people reported more past suicidal thoughts and attempts, feeling like a burden, feeling like they don’t belong and traumatic life events. But I’ve also found that these experiences are less strongly associated with reporting lifetime suicidal thoughts or behaviours than in not autistic people. This could mean that the model is less useful and different risk factors influence suicidal thoughts and behaviours in autistic adults. Or it could even mean that burdensomeness or not belonging are everyday experiences for autistic people. And there could be another reason: questionnaires designed to measure feeling like a burden or not belonging in not autistic people may be differently understood by autistic people.
3. How do we measure suicide risk in autistic people?
We know from research that standardised mental health measures may bring inaccurate results in autistic adults [5]. Autistic characteristics can mean that autistic people respond differently to questionnaires designed for not autistic people: they may interpret information literally or find it difficult to infer past or future events. They may find it difficult to detect and express their own internal emotional state: termed ‘alexithymia’ – this is much more common in autistic than not autistic people. Mental health symptoms may mirror autistic characteristics, such as reduced eye contact, limited social network or disrupted sleep. Emotional distress in autistic people may be observed through changes in sleep pattern and special interests, and agitation not captured by current tools. These factors all affect how autistic people are referred to and assessed by mental health services and how accurately we can identify suicide risk. Summarised in a systematic review recently, we can conclude that we don’t yet have a suicide risk measure that we know accurately measures risk in autistic adults [5].
And measurement issues are relevant for the findings of my study too. The associations could be weaker in the autistic group because autistic people responded to the questionnaire items differently or they may experience belonging differently. The ITS questionnaires are designed for use in not autistic people and, as is typical, rely on abstract metaphor, loose rather than concrete language and theory of mind (the ability to infer mental states in others), which is known to be different in autistic people. To check my results, I will compare how people responded to the questionnaire items to see if this explains why the model appears to work differently in each group.
So, how do we move forwards from here?
In summary, we know that autistic people are more likely to engage in suicidal thoughts and behaviours, but there are no models to explain why and no measures to accurately capture risk. Moving forwards, we need to work with people who understand this. To return to my opening paragraph, when I describe my research to autistic people or those who live or work closely in alliance with them, they are entirely unsurprised; they are aware of high suicide rates and can see how suicidal thoughts and behaviours develop. I recently spent an afternoon with the autistic adults who support me in my PhD research. They described how autistic people experience life challenges, why they might identify suicide as a solution and why they’d be unlikely to tell anyone about it. It is a privilege as a researcher to have such committed partners in my research. However, they also told me that, if I asked other autistic people, I would get a different answer. For this reason, I have written this blog and recorded a video outlining my research findings and asking for ideas about what they might mean. Please send me any comments or ideas on Twitter (@MiraPel1), by email (peltonm@uni.coventry.ac.uk) or just talk to me if you see me at events.
Conclusion
As researchers we need to design research that takes as its starting point the experiences of autistic people and embeds this throughout the research process. In this way, we can produce research that provides the evidence policymakers and service providers need to really reduce suicide rates.
*Notes:
[A] My research refers to autistic individuals without intellectual disability who are reported to be at increased risk of suicide.
[B] We use the less stigmatizing term ‘condition’ rather than a ‘disorder’ to describe autism. We use the term ‘autistic people’ to reflect the preferences of the autistic community (Kenny 2016) [A] My research refers to autistic individuals without intellectual disability who are reported to be at increased risk of suicide.
References:
- Hirvikoski, T., Mittendorfer-Rutz, E., Boman, M., Larsson, H., Lichtenstein, P., & Bolte, S. (2016). Premature mortality in autism spectrum disorder. The British Journal of Psychiatry: The Journal of Mental Science, 208(3), 232. Retrieved from https://pdfs.semanticscholar.org/d4ca/e0b1efaaaf1e6d4ad452636ea6a898bb7e67.pdf
- Cassidy, S., Bradley, L., Shaw, R., & Baron-Cohen, S. (2018). Risk markers for suicidality in autistic adults. Molecular Autism, 9(1), 42-14. doi:10.1186/s13229-018-0226-4 Retrieved from https://molecularautism.biomedcentral.com/articles/10.1186/s13229-018-0226-4
- Pelton, M. K., & Cassidy, S. A. (2017). Are autistic traits associated with suicidality? A test of the interpersonal-psychological theory of suicide in a non-clinical young adult sample. Autism Research, 10(11), 1891-1904. doi:10.1002/aur.1828 Retrieved from https://onlinelibrary.wiley.com/doi/pdf/10.1002/aur.1828
- Griffiths, S., Allison, C., Kenny, R., Holt, R., Smith, P., & Baron‐Cohen, S. (2019). The vulnerability experiences quotient (VEQ): A study of vulnerability, mental health and life satisfaction in autistic adults. Autism Research, (000), 1-13. doi:10.1002/aur.2162 Retrieved from https://onlinelibrary.wiley.com/doi/pdf/10.1002/aur.2162
- Cassidy, S. A., Bradley, L., Bowen, E., Wigham, S., & Rodgers, J. (2018). Measurement properties of tools used to assess suicidality in autistic and general population adults: A systematic review. Clinical Psychology Review, 62, 56-70. doi:10.1016/j.cpr.2018.05.002 Retrieved from https://www.sciencedirect.com/science/article/pii/S0272735818300692

Mirabel Pelton (@MiraPel1) has a MSc in psychology and is currently a PhD Researcher at Coventry University and a Research Assistant at University of Birmingham looking at transition into psychosis (peltonm@uni.coventry.ac.uk).
*Featuring photo by Sharon McCutcheon on Unsplash.

1 thought on “3 things we should know about suicide in autistic adults”