
By Jessica Leather.
Psychological science has been at the centre of many people’s minds since the COVID-19 pandemic began, especially those in search of effective public health messaging and coping strategies. Recently an expert panel in psychological science highlighted mental health as a research priority, due to the shifting social conditions and economic instability resulting from international lockdown measures [1]. Although the extent of the mental health impact from COVID-19 is not yet known, there are concerns that the pandemic may exacerbate risk factors for self-harm and suicide [2]. Now more than ever, there is a serious need to ensure there are effective resources to manage self-harm, in order to address existing gaps between policy and service provision [3].
I am about to start my final year as a PhD student funded by the Greater Manchester Patient Safety Translational Research Centre, where I have been working to address the implementation gap between the national guidelines for self-harm in England and Wales and professional practice. I have been engaged in several behavioural science projects since completing my masters in health psychology in 2017, ranging from the development of a tool to quantitatively measure alcohol expectancies, to the qualitative evaluation of a bowel cancer screening project. ‘Behavioural science’ encompasses a broad spectrum of research; it often involves the use of models to understand or predict certain behaviours, while employing appropriate techniques to change people’s behaviour. While this typically refers to public or patient health-related behaviours, my research focuses on understanding and intervening in the behaviour of healthcare professionals. More specifically, I aim to target healthcare professionals that are likely to encounter patients who self-harm, so they can better implement national guidance for self-harm.
To achieve this, I took a ‘ground-up’ approach by using an existing framework of behaviour change to inform the design of a behaviour change intervention. The national guidelines for self-harm in the United Kingdom suggest that all healthcare professionals should have adequate training to manage self-harm, that risk screening tools should not be used and that medical treatment and psychosocial assessment should be offered to all patients who have self-harmed. However, the factors that enable or prevent staff to implement national guidance when they encounter a patient were unclear. I designed an online survey to find out which barriers and enablers were associated with implementation of the guidelines by using the Behaviour Change Wheel (BCW) to develop an intervention [4].
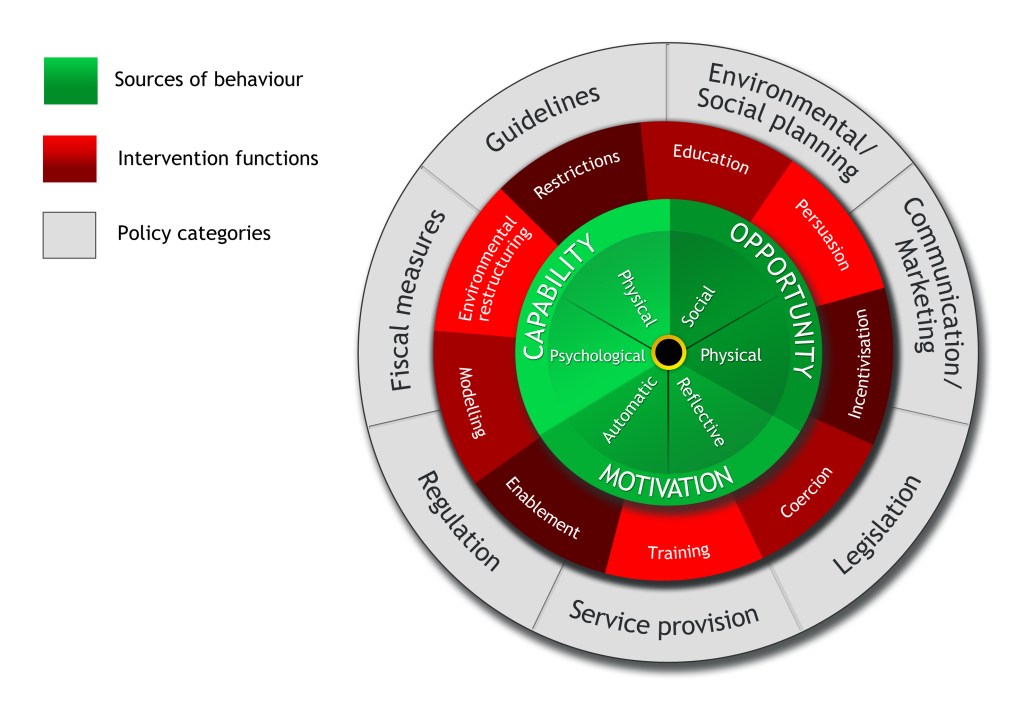
While the COM-B framework is often used in isolation to understand behaviour, it is intended for use as part of a wider framework of intervention development. The ‘active ingredients’ of interventions are Behaviour Change Techniques (BCTs): to date there are 93 different BTCs that can be used to change behaviour [5]. The BCW has categorised these techniques into nine sets of intervention functions, since each function (the red middle wheel, Figure 1) can be used to target one or more of the COM-B facets (the green central wheel, Figure 1). For example, environmental restructuring (e.g.: interventions that change an individual’s environment) has been identified as an effective intervention category to target automatic motivation (e.g.: habit) [4]. One of the BCTs in the environmental restructuring category is ‘habit formation’. An exemplar intervention to target automatic motivation could promote habit formation through the use of prompts (e.g.: healthcare professionals could be prompted once a month to re-read the self-harm guidelines). The final part of the wheel dictates how an intervention will be implemented at a policy level. For example, to effectively change services for self-harm there needs to be appropriate service provision in place, so any interventions would need to be produced with the input of the services they are intended to be used by.
This blog has provided a whistle-stop tour of behaviour change intervention development, but I must emphasise that my project targets only one facet of self-harm behaviour; There is a need for more projects using behavioural science methods to address the needs of patients who self-harm. My colleagues in the Behavioural Science unit of the NIHR Greater Manchester Patient Safety Research Centre are developing a tool (with involvement from a PPI panel) for use by patients to reduce self-harm through the creation of if-then contingency plans, also known as ‘implementation intentions’ (e.g.: If I feel the urge to self-harm, then I will do something else). Again, this project employs just one of the 93 behaviour change techniques, which demonstrates the enormous potential scope of research to change self-harm behaviour at the patient, service-provider, and policy level [5].
References:
-
- O’Connor, D. B., Aggleton, J. P., Chakrabarti, B., Cooper, C. L., Creswell, C., Dunsmuir, S., … Armitage, C. J. (2020). Research priorities for the COVID-19 pandemic and beyond: A call to action for psychological science. British Journal of Psychology, 1–27. https://doi.org/10.1111/bjop.12468
- Gunnell, D., Appleby, L., Arensman, E., Hawton, K., John, A., Kapur, N., … Yip, P. S. (2020). Suicide risk and prevention during the COVID-19 pandemic. The Lancet Psychiatry, 7, 468–471. https://doi.org/10.1016/S2215-0366(20)30171-1
- Kapur, N. (2020). Services for self-harm: progress and promise? The British Journal of Psychiatry, (2020), 1–2. https://doi.org/10.1192/bjp.2020.104
- Michie, S., Atkins, L., & West, R. (2014). The Behaviour Change Wheel: A guide to designing interventions. (1st Editio.). Great Britain: Silverback Publishing.
- Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., … Wood, C. E. (2013). The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Annals of Behavioral Medicine, 46(1), 81–95. https://doi.org/10.1007/s12160-013-9486-6

Jess Leather (@JessZLeather) is a PhD student funded by the NIHR Greater Manchester Patient Safety Translational Research Centre at The University of Manchester. Email: jessica.leather@manchester.ac.uk
*Featuring Photo by Dylan Gillis on Unsplash.
